State of the Art and Science
Aug 2014
Medicine and the visual arts stem from essential human activities: learning about and taking care of our fellow humans and communicating with them. The intent of this article is to elucidate and describe therapeutic applications of art making in the elderly population, particularly those affected by dementia.
A three-axis model provides a frame for organizing the interactions between medicine and the visual arts. Longitudinally, visual functioning is part of an individual’s life from infancy through old age. We learn about the world through visual stimuli from early on and we continuously receive, process, and produce visual information (e.g., in the process of nonverbal communication). We can think of the visual arts as a subset of all visual functioning.
Cutting across the visual functioning axis at each life stage, visual art activities may be part of what people do for education, recreation, work, and self-expression and communication. Art activities can help develop cognitive abilities including visuospatial and attentional capacity, abstract thinking, and fine motor skills, all involved in the executing of an art project. We can then think of art activities along this second axis as contributing to the individual’s development of cognitive reserve, brain plasticity, and resilience.
This takes us to the third axis, where I place the health-illness continuum and medical care: inasmuch as they contribute to cognitive and emotional development, connection with others, and experience of joy, art activities help promote and maintain health. Once illness strikes, art activities can be part of the therapeutic tool set and assist in health restoration and rehabilitation.
I am going to expand on the function that art activities can serve among the elderly population. The enjoyment of the arts is important to many healthy senior citizens who attend art classes at senior centers and visit art museums. They may augment the skills that older persons retain, enabling them to make meaningful expressions [1] and promoting social and emotional growth [2]. In the increased focus on the building of cognitive reserve and the prevention of cognitive decline and dementia, participation in cognitive and leisure activities is emerging as one of the avenues to maintaining and developing cognitive skills in older age [3, 4]. Art activities are well suited to serve this function: they can be fun and social, and they promote learning. Importantly, they engage most brain circuits involved in our day-to-day activity.
Two functionally specialized pathways are essential for the processing and production of visual information [5]. The ventral visual pathway, with occipitotemporal localization, is involved with recognizing what we see. In art, we may then use our internal visual representations of people, animals, and objects to depict them in paintings and drawings. The dorsal stream, with occipitoparietal localization, allows us to perceive where an item is located in space and to see a scene as a whole. We apply these functions when we look at a painting and when we organize the composition of an art piece. The dorsal visual pathway also allows us to understand spatial locations so that we can act in space [6]. The language neurocircuits participate in the interpretation and depiction of symbolic, language-based concepts in visual form in a painting. The dorsolateral prefrontal cortex helps with the planning and organization of an artistic project. The frontal cortex may also have an inhibitory role in creativity [7]. The cortical and subcortical motor areas, along with the somatosensory pathways, are involved in skillful manipulation of art tools. Art viewing and creating also engage the vast neurocircuitry responsible for emotional processing, regulation, and expression.
In the setting of medical and psychiatric illness, art can be an excellent therapeutic tool and may assist in rehabilitation [2]. In the presence of degenerative brain illness, brain lesions change the nature of the art patients produce. The art of those with Alzheimer disease generally shows a gradual decline that parallels the decline of other cognitive abilities [8, 9]. In contrast, some patients with frontotemporal dementia (FTD), especially those with left anterior degeneration and preserved posterior parietotemporal regions, may temporarily acquire new artistic skills [10, 11].
Many individuals with dementia participate in art therapy activities in adult day programs, assisted living facilities, and nursing homes [12]. The Alzheimer’s Association Memories in the Making Art Program has assisted in developing some of these efforts [13]. Several art museums, including the MFA in Boston and MOMA in New York City, have held art programs for people with dementia and their caregivers; such programs tend to succeed as measured by engagement, communication, and pleasure for the participants [14].
Art activities can be part of a plan to manage agitation and other behavioral problems in the demented elderly. Visual creativity can help these patients maintain communication with others, including their loved ones, when other forms of cognitive functions are markedly impaired. A neurologist and I integrated neurological and psychiatric care, art therapy, and verbal psychotherapy in the treatment of one of our patients, a professional artist who developed corticobasal degeneration in her fifties [15]. While hers was a case of early-onset dementia, many of the principles we used in her treatment can be applied to patients with late-onset presentation. She came to our cognitive and behavioral neurology clinic due to gradually progressive difficulties in her visuospatial functioning. Her parietal lobes—especially on the right hemisphere—were significantly affected. In consequence, her dorsal visual pathway, which is fundamental in perceiving and depicting space and in making art, was clearly impaired.
In the few years prior to her diagnosis she had been immersed in her work, creating a series of abstract landscapes (figure 1).
Figure 1.

With the decline in her capacity to represent tridimensional space, her paintings acquired a flatter quality (figure 2).
Figure 2.

She had drawn a number of urban landscapes (figure 3) and, when no longer able to draw perspective, she created “new” versions by making collages with pieces from her older drawings (figure 4).
Figure 3.
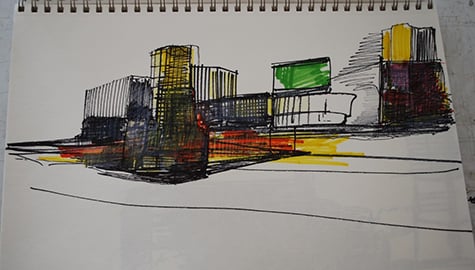
Figure 4.

By the time she first saw us, she had completely stopped making art, which was a source of great distress for her. I met with her periodically at her home-based art studio. With a neurological understanding of her illness, her neurologist and I were able to design specific art therapy interventions that contributed to her preserved functioning and helped develop compensatory strategies for her deficits. The therapeutic benefits of this interdisciplinary approach could not have been achieved otherwise. Our interventions, while not able to alter the ultimate course of the illness, significantly improved her quality of life, reawakened her capacity to exercise her identity as an artist, brought back her enjoyment of art making, and provided a sense of hope.
Wadeson H. Residential care for the elderly. In: H Wadeson, ed. The Dynamics of Art Psychotherapy. New York: Wiley & Sons; 1987: 228-233.
MacPherson S, Bird M, Anderson K, Davis T, Blair A. An art gallery access programme for people with dementia: ‘You do it for the moment.’ Aging Ment Health. 2009;13(5):744-752.



