Viewpoint
Sep 2023
Peer-Reviewed
The nature and scope of palliative psychiatry and associated ethical implications are debated in the literature. This article examines conceptual limitations of extant accounts of palliative psychiatry, with a focus on psychopharmacological practice, and suggests that modifiable and unmodifiable psychiatric illnesses exist on a spectrum along which broader or narrower palliative psychiatric care approaches can be outlined. The article also discusses how these approaches intersect with questions about whether and to what extent psychiatric medications have symptom-reducing or disease-modifying effects. The discussion leads to the conclusion that clinicians are ethically obliged to distinguish among and clearly formulate goals of care in a dynamic and ongoing process of shared decision making with patients.
Palliative approaches in psychiatry have received increasing attention in recent years. Although existing work has attempted to define the boundaries of what constitutes palliative psychiatry,1,2 many conceptual issues and their ethical implications remain in need of further clarification. In this article, I examine the conceptual limitations of existing accounts of palliative psychiatry, focusing on the practice of psychopharmacology, and address these limitations by emphasizing modifiable and unmodifiable aspects of the illness in relation to other distinctions. I also discuss how this approach intersects with ongoing debates about whether psychiatric medications have symptom-reducing or disease-modifying effects.
Although palliative medicine was initially focused on end-of-life care, it is currently conceptualized as relevant to all chronic, serious, or life-threatening medical conditions, and it can be offered concurrently with curative treatments. The World Health Organization defines palliative care as “an approach that improves the quality of life of patients (adults and children) and their families who are facing problems associated with life-threatening illness. It prevents and relieves suffering through the early identification, correct assessment and treatment of pain and other problems, whether physical, psychosocial, or spiritual.”3 Palliative psychiatry applies the principles of palliative care to serious and persistent mental illness. Unlike many chronic conditions in general medicine, the etiology and pathophysiological mechanisms of various psychiatric conditions remain poorly understood, and our ability to modify the mechanisms directly involved in pathophysiology remains limited. The boundary between routine psychiatric care and palliative psychiatric care has accordingly proven to be more elusive than that between palliative and general medicine.
This demarcation problem brings uncertainty to the practice of palliative psychopharmacology, with attendant ethical consequences. If we present palliative treatment as curative, we generate an erroneous idea that the etiological causes or the causal mechanisms of the distressing and impairing states are being addressed. By the same token, adopting a palliative approach prematurely or inconsistently—for instance, by opting for symptomatic pharmacological relief without addressing modifiable psychosocial factors that causally contribute to the persistence and severity of the psychiatric illness or by failing to recognize that one has shifted from a curative to a palliative approach—is ethically significant, since doing so may result in an inadvertent narrowing of the focus of clinical care, with suboptimal outcomes. How, then, to conceptualize the relationship between psychiatry and palliative care?
On the relationship between psychiatry and palliative care, Trachsel et al have noted that “several clinical approaches in contemporary psychiatry can already be considered palliative, as they aim at reducing symptoms and suffering from mental illness rather than seeking to achieve disease remission or disease modification.”1 Balon et al have gone further in raising the possibility of characterizing psychiatry itself as a form of palliative care: “in many aspects, psychiatry itself is a form of palliative care because psychiatric treatments are frequently not curative.”4 Other proponents of palliative psychiatry, however, have recognized that this suggestion is too expansive2 because it blurs the distinctive ways in which palliative care prioritizes quality of life and harm reduction strategies over other clinical goals in the management of chronic, serious, or life-threatening conditions and have proposed that the term palliative psychiatry be used to describe care of those only with severe and persistent mental illness (SPMI). Rather than characterize psychiatry itself as a form of palliative care, Westermair et al have elaborated on narrow and broad notions of palliative psychiatry: “palliative psychiatry in a narrow sense refers to the provision of end-of-life care for persons dying from a mental illness. An example is hospice care for persons dying from anorexia nervosa…. [P]alliative psychiatry in a broad sense refers to all approaches aiming at improving quality of life by means other than reduction of SPMI symptoms, namely harm reduction and relief of suffering.”2 My interest here is in psychopharmacology in palliative contexts, so I will not focus on other interventions, such as various modalities of psychotherapy, which have an essential role to play in palliative psychiatry in the broad sense.
We can extract 2 sorts of views about palliative psychopharmacology implicit in the quotations above: one view, exemplified by Trachsel et al and Balon et al, focuses on whether medications are symptom reducing or disease modifying and, to the extent that psychiatric medications are symptom reducing, maintains that they are potentially palliative (provided they are used in the appropriate clinical context). According to the other view, exemplified by Westermair et al, medications are curative if used with the goal of symptom reduction and palliative if the goal is not symptom reduction but improved quality of life. As I will explain, both approaches encounter significant limitations.
There are different paths to improving quality of life. Some involve modifying the central pathophysiology of the illness, some involve symptom reduction without disease modification, and some involve neither symptom reduction nor disease modification. It has been argued that psychiatric medications, for the most part, are symptom reducing (akin to analgesics and antipyretics) and not disease modifying.5
Ghaemi, a notable proponent of the distinction in psychiatry between symptom-reducing and disease-modifying interventions, defines disease modification partly biologically and partly clinically.5 Biological disease modification involves altering the pathophysiology of the disease process. Lipid-lowering drugs and antihypertensive drugs in cardiovascular illness are examples. Clinical disease modification involves improvement in the course of illness and mortality. Examples include reduced risk of future myocardial infarctions and malignant recurrences. Ghaemi argues that most psychiatric medications do not satisfy either criterion and that medication classes such as antidepressants and antipsychotics, while effective in reducing symptoms, do not modify the etiology or the long-term course of the illness.5
The boundary between routine psychiatric care and palliative psychiatric care has accordingly proven to be more elusive than that between palliative and general medicine.
Ghaemi, building on earlier work with Selker,6 calls for evidence of disease modification to meet a certain threshold.5 For instance, this would require that reduction of future episodes of illness be demonstrated in randomized trial designs other than “randomized discontinuation” trials,6 that evidence for modification of long-term course should not come only from observational studies, and that evidence for neuroprotection should involve a range of neuroprotective markers and be shown in vivo in humans. There is evidence that antidepressants do reduce risk of future relapse of depression7 and enhance neuroplasticity and neurogenesis,8 that early treatment of psychosis modifies long-term course,9 and that antipsychotics lower mortality,9 but this body of evidence doesn’t meet the criteria laid out by Ghaemi.5 In other words, there is evidence suggestive of disease modification, but the scientific debate on this issue extends to what threshold of evidence is sufficient for us to accept that disease modification is taking place. There are additional considerations, such as the hypothesized “kindling” phenomenon in mood disorders, according to which each episode of a mood disorder reinforces brain pathways that render the individual more susceptible to a future episode. It is hypothesized that early treatment may modify this progression.10 While I do consider neuroscientific hypotheses and observational evidence in support of disease modification to be important and relevant, it is not my intention to settle the matter here in either direction; we only have to note that uncertainty about the evidence complicates labeling an intervention as disease modifying or symptom reducing. In particular, if we link the palliative status of psychopharmacological treatment to whether or not it is disease modifying, we’d have to acknowledge that there is a lack of scientific consensus on the matter, precluding us from saying with certainty whether the intervention is palliative or not. This circumstance prompts us to consider other standards by which psychiatric treatments may be judged to be palliative.
As noted, a superficial impression is that palliative psychopharmacology involves the use of symptomatic agents while a curative approach involves disease-modifying agents, but this distinction is misleading. The curative-palliative distinction is orthogonal to the symptomatic-disease-modifying distinction, and medications used for palliative purposes may be either symptomatic or disease modifying, depending on the context in which and the purpose for which palliative care is being offered. For instance, chemotherapy targets malignant cells directly and is disease modifying, but palliative chemotherapy is often used to improve symptoms or quality of life in advance-stage cancers.
Some authors, such as Westermair et al,2 have distinguished curative psychiatry from palliative psychiatry by characterizing symptom reduction as a curative goal in psychiatry: “whereas curative psychiatry strives at improving quality of life by way of symptom reduction or even complete remission, palliative psychiatry aims at relieving suffering and thus improving quality of life directly by working around irremediable SPMI symptoms.”2 This characterization of the goal of symptom reduction as curative in psychiatry is problematic, since it doesn’t hold for palliative medicine generally, as improving quality of life via targeting symptoms (such as pain or shortness of breath) is a recognizably palliative goal.11
In my view, the relevant distinction in palliative psychopharmacology is not etiology vs symptoms or symptoms vs quality of life, but rather modifiable vs unmodifiable aspects of illness in relation to quality of life—aspects that may be either etiological mechanisms or symptoms. My use of the term unmodifiable is also intended to describe situations in which we have decided not to modify an aspect of the illness in the interest of prioritizing quality of life. The essence of palliative care, I suggest, is when we are forced to work around an aspect of the illness to enhance quality of life. This aspect will be different in different situations. In prototypical instances of terminal illness in palliative medicine, the aspect that must be worked around is the inevitability of death from illness progression. In conditions such as advanced chronic obstructive pulmonary disease, it is the unalterable nature of pathophysiological changes in the lungs; symptoms have to be improved by working around the damaged lung tissue. In palliative psychiatry as envisioned by Westermair et al,2 it is the persistent symptoms of SPMI, such as chronic hallucinations or persistent functional disability that respond inadequately to antipsychotic treatment.
The notion of “unmodifiable” presented here has similarities to the notion of “futility,” which has been applied to palliative psychiatry by Levitt and Buchman.12 Invoking futility implies that the nature of the situation is such that available interventions will almost certainly have no benefit, either because of the terminal nature of the condition or because treatment resistance has made the dynamic risk-benefit ratio unfavorable. The notion of unmodifiable complements the notion of futility and is not in conflict with it; it is a broader notion that highlights that aspects of an illness may be unmodifiable even in the absence of futility (eg, cognitive impairment in first-episode schizophrenia), just as aspects of even a terminal illness are modifiable palliatively (eg, reducing acute anxiety or panic with benzodiazepines).
I elaborate on the notions of modifiable and unmodifiable in the Table by applying them to various aspects of psychiatry and palliative care.
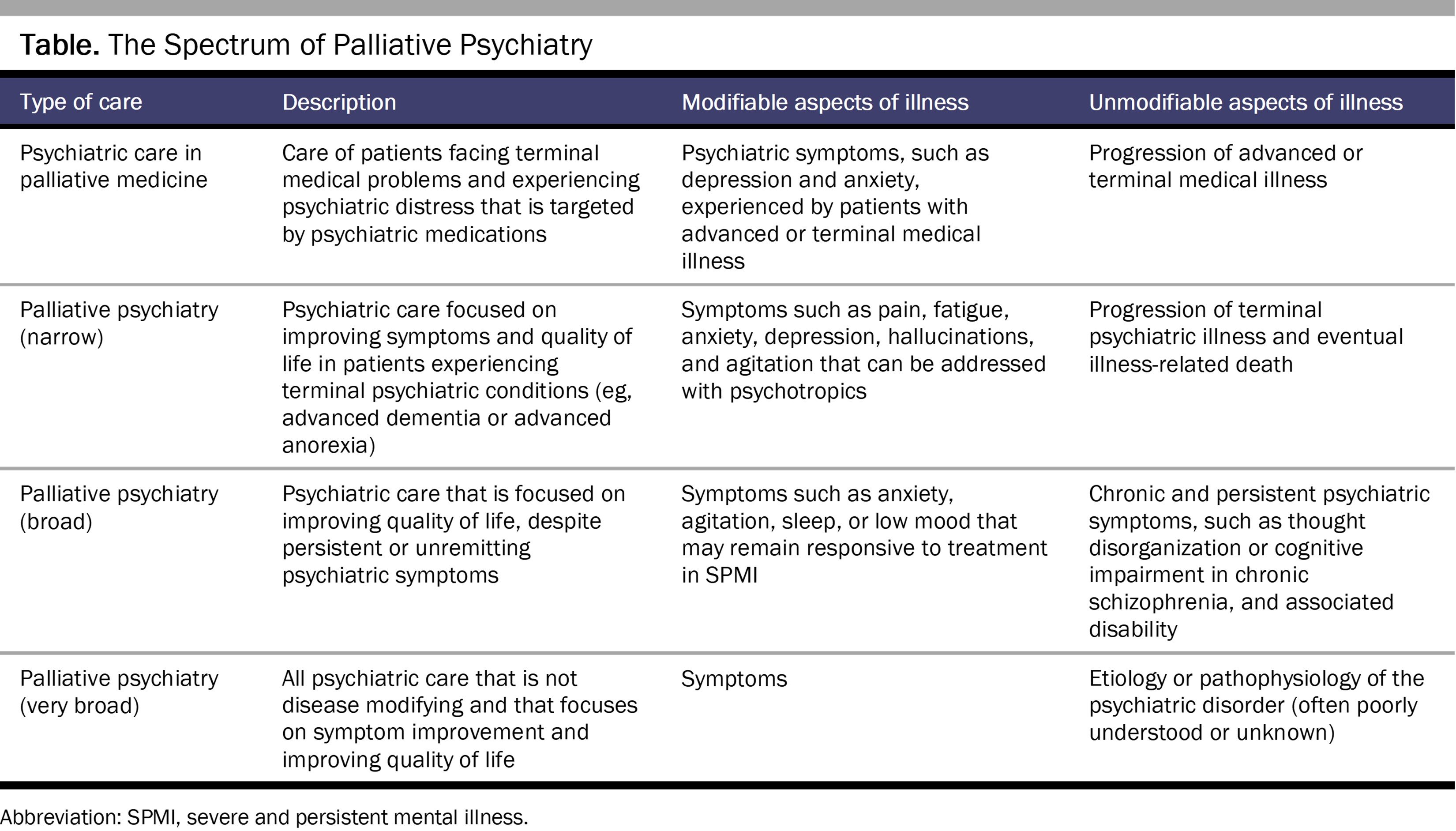
We can make further fine-grain distinctions as well. For instance, the severity of symptoms may be modifiable but not their persistence (for instance, hallucinations may become less intense or less frequent but otherwise continue to be experienced); acute episodes may be modifiable but not their recurrence (for instance, for some patients, antidepressant medications may alleviate an active episode of depression but may not successfully prevent future episodes). These examples serve to illuminate the dimensionality of palliative goals and their overlap with curative goals. What distinguishes any particular instance of care as palliative is an emphasis on quality of life and an acceptance of the unmodifiable aspects of an illness. The unmodifiable aspects of an illness are also not predetermined. The traditional instances of palliative care are recognizable with reference to treatment contexts wherein the unmodifiable aspects are obvious and stable—as in advanced or terminal physical illness—but as the application of palliative approaches extends to other treatment settings, what is characteristic of palliative care may be less obvious. Conversely, unmodifiability does not necessarily imply that the care provided is automatically palliative. Where exactly we draw the line on this spectrum between modifiable and unmodifiable aspects of illness—the threshold at which the characterization of our clinical approach begins to shift from curative to palliative—is a pragmatic matter.
Broader or narrower notions of “palliative” offer correspondingly different advantages and disadvantages. Very broad notions (eg, that routine psychiatric care itself is a form of palliative care) may be unhelpfully broad compared to narrower notions that keep the focus on improving symptoms and quality of life in cases of treatment resistance, SPMI, or futility. Consider the use of intravenous ketamine (or intranasal esketamine)13 to treat severe and persistent depression that has proven refractory to standard treatments. If the goal is remission or significant alleviation of depressive symptoms, this intervention will not typically qualify as palliative. However, consider other possible outcomes of treatment: ketamine temporary relieves depression but the depression inevitably returns (unmodified recurrent course); ketamine reduces depression severity but the depression persists otherwise (unmodified chronicity and persistence); or the depression is unaltered but the psychoactive experiences (eg, euphoria, dissociation) make depression more tolerable for the patient (unmodified symptoms). If treatment is continued in the case of such outcomes, these goals can reasonably be considered palliative. Whether ketamine treatment increases or decreases quality of life and by what pathway can’t be determined in advance for a particular individual. Similar considerations can also apply to other psychotropics, such as antidepressants for which it is possible that different individuals experience benefit via different pathways.14 A consequence of this view is that clinicians have an ethical imperative to distinguish among and clearly formulate goals of care in a dynamic and ongoing process of shared decision making with patients.
The importance of how psychiatric treatment is conceptualized by patients was recently illustrated by the “chemical imbalance” debate in the public.15 Many individuals in the public who erroneously thought that depression is caused by a serotonergic deficiency and that antidepressants are normalizing serotonin levels were upset to learn that this explanation was fallacious.16 At least some of the causes of severe, persistent depression are contextual and relational and not addressed by pharmacological treatment. If a pharmacological treatment is being employed palliatively, both the clinician and the patient need to be aware of that. Understanding that treatment is palliative is an issue that pertains not only to informed consent and nonmaleficence, but also to hermeneutic justice. Gaining more clarity on what their treatment seeks to modify and what it leaves unmodified will help patients better understand the nature of their psychiatric care and will ensure that clinicians do not ignore potentially modifiable causes.
Trachsel M, Irwin SA, Biller-Andorno N, Hoff P, Riese F. Palliative psychiatry for severe persistent mental illness as a new approach to psychiatry? Definition, scope, benefits, and risks. BMC Psychiatry. 2016;16(1):260.
Palliative care. World Health Organization. August 5, 2020. Accessed October 27, 2022. https://www.who.int/news-room/fact-sheets/detail/palliative-care
Marchionatti LE, Antonelli-Salgado T, Erthal IN, et al. Bipolar disorder treatment according to illness trajectory: a systematic review of clinical trials. Psychiatry Res. 2022;312:114572.
Levitt S, Buchman DZ. Applying futility in psychiatry: a concept whose time has come. J Med Ethics. 2021;47(12):e60.
Love S. The new study on serotonin and depression isn’t about antidepressants. Vice. July 22, 2022. Accessed October 27, 2022. https://www.vice.com/en/article/88qge4/the-new-study-on-serotonin-and-depression-isnt-about-antidepressants-chemical-imbalance
Ratnayake S. Why has the misleading “chemical imbalance” theory of mental illness persisted for so long? Slate. August 4, 2022. Accessed October 27, 2022. https://slate.com/technology/2022/08/ssris-chemical-imbalance-depression.html



