Medical Education
Mar 2022
Peer-Reviewed
Medical education is limited to the biomedical model, omitting critical discourse about racism, the harm it causes minoritized patients, and medicine’s foundation and complicity in perpetuating racism. Against a backdrop of historical resistance from medical education leadership, medical students’ advocacy for antiracism in medicine continues. This article highlights a medical student-led antiracist curricular effort that moves beyond a biomedical model and uses abolition as the guiding framework in the creation process, the content itself, and iterative reflection through further study and dissemination.
In 1971, Rodney G. Hood, one of the first Black medical students at the University of California, San Diego, protested a psychology professor’s lecture about the intellectual inferiority of Black people.1 The lecturer falsely claimed that because the Eurocentric intelligence quotient (IQ) was inherited, educating Black people was a waste of resources. The future Dr Hood was told by medical school administration that the lecturing professor was in his rights because of “scientific enlightenment and freedom of speech.”1
Fifty years later, medical students of color continue to face the same racism and White supremacy that Hood experienced.2 Racism, a system of structuring opportunity and assigning value based on race,3 undergirds minoritized groups’ underrepresentation in medicine,4,5 inequitable grading and evaluations,6,7,8 and exclusion from honor societies.9 White supremacy, a political, economic, and cultural system in which White people overwhelmingly control power and material resources, asserts White superiority at every turn.10 An important manifestation of White supremacy is the overwhelming whiteness of medical education leadership, from medical school deans11 to journal editors.12
Medical education perpetuates racism by treating race as a biological rather than a social construct; asserting that Black, Indigenous, and people of color (BIPOC) are biologically different, unusual, or inferior; and maintaining medicine’s complicity in pervasive racial health inequities.13,14,15,16 When students name racism in medical institutions, the White hegemony of medical leadership silences their voices in myriad ways—placating them without committing to real structural change, gatekeeping antiracism efforts, and gaslighting their lived experiences. Students cannot depend on medical schools to provide the antiracist medical education they deserve.
In 2020, through a grant from the American Academy of Family Physicians Emerging Leader Institute to one of the authors (R.M.M.), we, as a collective, decided to create antiracist medical curricular content that would be accessible to any student, health professional, or institution nationwide that wanted to engage in antiracism. We utilized our lived experiences as Black, Punjabi-Sikh, Filipino, and Mexican American people who have endured racism to create the antiracist education that we and our communities deserve. We aim to educate a new generation of physicians and to reeducate physicians who have harmed our family members through personally mediated racism and complicity with systemic racism.
Our content and process were rooted in abolition, a term historically applied to the movement to end slavery and more recently to the movement to vanquish the prison-industrial complex.17 As Iwai, Kahn, and DasGupta write: abolition medicine “interrogate[s] the upstream structures that enable downstream violence, like police brutality.”18 It reimagines “the work of medicine … as an antiracist practice” by abolishing diagnostic tools and treatment guidelines that reinforce biological race, calling for desegregation of the medical profession and demanding reparations for communities devastated by medical experimentation.18
Abolition in the curricular development process. Rooting our process in abolition centered on rejecting the White supremacy culture central to medical training19 and fostering collective solidarity to bolster our shared efforts. Instead of pursuing perfectionism with urgency, we built a culture of appreciation and shared learning and prioritized reflective pauses. In place of individualism, we embraced our plurality, which enabled us to enlighten one another on where we would otherwise have had blind spots. We did not shy away from our tensions and instead dove into the conflicts within and amongst ourselves. We honored the different realities that have been so long erased by “objectivity” and worship of the quantifiable and of the written word.
We were humans first, beginning our meetings by checking in emotionally before delving into our work, thereby creating space for grief, frustration, and anxiety. We established an ongoing, dynamic system of informed consent for the emotional labor and spiritual work that antiracism requires. This informed consent process included periodically revisiting our individual involvement with the project, reflecting on whether our effort felt life-giving or draining, and determining whether we wished to continue or to take a break. We specified agenda items prior to each meeting, allowing participants to come and go as needed. We replicate this approach in our curriculum, which outlines how to create a safe learning environment that encourages learners to step away as needed. As individuals came and went due to life tragedies, we did our best to be loving and accepting, not punitive. With relationships grounded in collective trust, we avoided required attendance to minimize minority taxation and encouraged individuals to participate as their bandwidth allowed. By eliminating hierarchy and centering process over product, we began our separation from the White supremacy culture indoctrinated in us by our medical training.
Abolition in medical curricular content. Most undergraduate medical education curricula are grounded in the biomedical framework, variably including health disparities data, social science principles, and, rarely, critical race theory. These limitations are magnified in graduate medical education, in which didactic time is limited. Instead of reforming the fundamentally broken curricula that exist, we redirected our energy towards creating something radical, bold, and new.
We began by rejecting the sanitized, apologetic frameworks centering White comfort and passivity, such as racial disparities and cultural competency. Instead, we rooted our work in abolition, critical race theory, and decolonization to emphasize racism and White supremacy’s ordinariness, toxicity, and productivity for those in power (see Supplementary Appendix). These radical frameworks, each of which we explain in the curriculum itself, guided us in highlighting the carceral logic permeating our “caregiving” profession. This logic includes punitive, degrading, and patient-blaming language, such as “noncompliant,” and clinical care’s direct ties to institutions like policing and the child welfare system. Explicitly stating this logic and connecting it to the profession’s deep ties to slavery helped us eliminate the euphemisms obscuring the racist violence that killed Dr Susan Moore and Daniel Prude.20,21
Antiracist medical education renders the invisibility of Whiteness visible to highlight its role in upholding medical racism and preventing change.
Each of us led the development of an organ system-based module. Individually, we searched the materials that were left of our medical education. We compiled stories and data demonstrating decades of abuse of people of color by medical professionals and how medicine has perpetuated the oppression of our communities. Each module identifies key racial inequities pertaining to the organ system at hand and unpacks how they derive from the structural racism and institutionalized White supremacy forged by the legacies of slavery and settler colonialism. Together, we reflected on the evidence and identified 4 overarching themes permeating all modules: segregation and structural racism, racial essentialism and institutionalized racism, medical abuse and personally mediated racism, and medicine and the carceral state. We close each module by highlighting extensive antiracist strategies (clinical, research, otherwise) to challenge and dismantle racist practices.
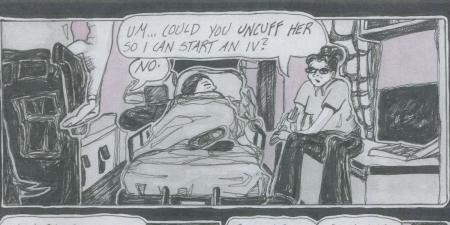
A clinical case woven throughout each module renders the brutality of racism and White supremacy palpable. One of the modules describes the experiences of X, a 17-year-old child who identifies as gender nonbinary and Mayan-Haitian biracial. They were brought into the psychiatric emergency department by police in 4-point restraints after their parents stated that they made suicidal comments. The module utilizes elements of X’s story to highlight the clinical coercion and racist abuse people of color face within the health “care” system. X’s story provides an entry point into the far-reaching impact of segregated schools and the legacy of overpathologizing BIPOC’s emotional distress in response to racism, White supremacy, and other systems of oppression. This narrative-based approach breathes humanity into statistics and guards against the intellectualizing and other defensive maneuvers preventing learners from implicating themselves in racism and other forms of oppression. The message to learners is clear: this is your story and your reality, too, and either you are part of the problem or you commit to being part of the change effort.
This content confronts the refusals of White supremacy—namely, its tolerance for perpetual violence and exploitation and its complacence in the face of a history of racial oppression that continues to shape the present.22 It renders the invisibility of Whiteness visible to highlight its role in upholding medical racism and preventing antiracist change. These modules reject sidelining antiracism to a lunchtime talk or a single lecture. Several hours long and requiring a half day or more, the modules are emotionally demanding and intellectually provocative to encourage interrogation of, rather than blind acceptance of, science as objective truth. As such, a significant amount of teaching is focused on creating the optimal space for transgressive learning. Furthermore, a detailed introduction module provides an overview of the key terms (eg, antiracism, oppression, racial essentialism), guiding frameworks (eg, critical race theory), and the 4 major themes permeating the modules.
Abolition in clinical practice. Our primary goal for this curriculum is positioning learners to undo racism within health care the minute they walk out the door—while anticipating White supremacist backlash along the way. By heightening their awareness of the racist beliefs, histories, policies, and structures in which we, as health care professionals, are complicit, the curriculum cultivates learners’ skills for making their home institutions antiracist. The case of X, for example, demonstrates how clinicians can prevent forced injection medication for “aggression,” connect families to community alternatives to calling the police, and draft compelling school letters of support to mitigate X’s risk of harm, violence, and punishment from the health care system and other institutions.
Remaining self-reflective, we recognize that abolition—to paraphrase Mariame Kaba23—is a series of a million different experiments each day and that we are destined to fail. Similar to how we continue to evaluate, adjust, and refine our modules, we do the same with our process of collaborative creation and implementation.
In the initial iteration of our project, our perspectives were limited based on our privileged positions within academic medicine. Recognizing the opportunity we missed, we are now inviting community members and patients to partake in the module-creating process. The abolitionist way of teaching is to flip the script and allow patients to guide our learning—for once—and to dissolve paternalism so that we can extend solidarity and build a movement.
As we move into the dissemination and implementation phase of our innovation, we now face the challenge of bringing an antiracist curriculum with an abolitionist orientation into the system of oppression that never would have condoned its creation. We continue to weigh the risks and benefits of organizational involvement and formalized research, knowing that many aspects of the ivory tower are diametrically opposed to equity and justice. We question the processes by which these materials would be “vetted” by faculty and professional organizations molded by the systems of oppression we seek to dismantle. As we interrogate the avenues through which this work is disseminated, we refuse to dilute our curriculum’s message or bend it to fit the reality of White supremacy for the sake of its acceptance. Recognizing that acceptance can be a challenge for a newly imagined antiracist curriculum, we are partnering with a medical school to ensure its practical application. Far from being forgotten, Hood’s legacy and lessons endure in our consciousness and strategy 50 years later.
Kwame Ture once said: “When you see people call themselves revolutionary always talking about destroying, destroying, destroying but never talking about building or creating, they’re not revolutionary. They do not understand the first thing about revolution. It’s creating.”23 It is in this spirit of reimagination and creation that we invite antiracist medical education’s abolitionist transformation.
BIPOC students’ and community members’ expertise, not faculty or administrators', fuels transformation in medical education. We urge BIPOC students to take their seats at the tables they build outside of the house of medicine. The harm prevented, solidarity cultivated, radical vision nurtured, and movement advanced when like-minded medical students link up is not only worthwhile but absolutely necessary. And there is no time to wait.
Hood RG. Commentary: I experienced racism at UCSD medical school 50 years ago. There’s still work to do. San Diego Union Tribune. July 7, 2020. Accessed April 25, 2021. https://www.sandiegouniontribune.com/opinion/commentary/story/2020-07-07/ucsd-medical-school-racism
Hlavinka E. Racial bias in Flexner Report permeates medical education today. MedPage Today. June 18, 2020. Accessed April 25, 2021. https://www.medpagetoday.com/publichealthpolicy/medicaleducation/87171
Lett LA, Murdock HM, Orji WU, Aysola J, Sebro R. Trends in racial/ethnic representation among us medical students. JAMA Netw Open. 2019;2(9):e1910490.
Ross DA, Boatright D, Nuñez-Smith M, Jordan A, Chekroud A, Moore EZ. Differences in words used to describe racial and gender groups in medical student performance evaluations. PLoS One. 2017;12(8):e0181659.
Chadha N, Kane M, Lim B, Rowland B. Towards the abolition of biological race in medicine and public health: transforming clinical education, research, and practice. Institute for Healing and Justice in Medicine. Accessed June 20, 2021. https://www.instituteforhealingandjustice.org/
Davis AY. Race and criminalization: Black Americans and the punishment industry. In: Lubiano W, ed. The House That Race Built. Vintage Books; 1998:264-279.
Okun T. White supremacy culture. Dismantling Racism. Accessed June 20, 2021. https://www.dismantlingracism.org/uploads/4/3/5/7/43579015/okun_-_white_sup_culture.pdf
Eligon J. Black doctor dies of COVID-19 after complaining of racist treatment. New York Times. December 23, 2020. Accessed April 25, 2021. https://www.nytimes.com/2020/12/23/us/susan-moore-black-doctor-indiana.html
Gold M, Closson T. What we know about Daniel Prude’s case and death. New York Times. April 16, 2021. Accessed April 25, 2021. https://www.nytimes.com/article/what-happened-daniel-prude.html
Gravlee C. How whiteness works: JAMA and the refusals of White supremacy. Somatosphere. March 27, 2021. Accessed April 25, 2021. http://somatosphere.net/2021/how-whiteness-works.html/
Kaba M. We Do This ’Til We Free Us: Abolitionist Organizing and Transforming Justice. Haymarket Books; 2021.