Why Consider Self-Sampling for Cervical Cancer Screening in Low- and Middle-Income Countries?
Victoire Fokom Defo, MD and Joël Fokom Domgue, MD, MPH
AMA J Ethics. 2020;22(2):E116-125. doi:
10.1001/amajethics.2020.116.
Abstract
Molecular detection of high-risk human papillomavirus (HPV) in genital cells is being widely endorsed as a preferred tool for cervical cancer screening globally. In low- and middle-income countries (LMICs) where cervical cancer remains a leading killer, HPV testing is an appealing, accessible alternative to traditional cytology (ie, Pap smear) screening that enables women to self-collect specimens. This article examines self-sampling and its suitability as a strategy for cervical cancer prevention in LMICs that would promote equitable access to cervical cancer screening.
Introduction
Cervical cancer is preventable but remains one of the most commonly diagnosed cancers around the world.1 More than 85% of new cases occur in low- and middle-income countries (LMICs), which bear 90% of the burden of cervical cancer mortality,2 primarily due to low coverage rates for cervical cancer screening services.3 Since cervical cancer is preceded by infection with high-risk strains of the human papillomavirus (HPV), screening tests have been developed to detect the presence of these high-risk HPV types in cervical cells. HPV testing is more sensitive than the traditional cervical cancer screening modality, cytology (ie, Pap smear),4 which has been successfully used to reduce the burden of cervical cancer in high-income countries. Compared to cytology, HPV testing is less resource intensive and can be done using either a clinician-collected cervical swab or a specimen collected by the woman (self-sampling).
HPV self-sampling is an innovative technique for cervical cancer screening that empowers women by allowing them to collect their own specimen in private, at a time and place of their choosing and when and where they are comfortable. It has the potential to overcome many of the identified barriers to accessing cytology in LMICs. Specifically, self-sampling removes the need for a pelvic exam, clinic setting, and a trained clinician.5,6 This strategy not only is acceptable to both women and clinicians but also is adapted to hard-to-reach and rural communities with limited transportation options and distant health facilities.7 As a result, it can potentially improve access to and uptake of screening, particularly among underscreened women and LMIC populations.5,8 In view of the above, HPV self-sampling might reduce social inequalities in access to cervical screening services.
By respecting women’s privacy, self-sampling might encourage screening participation in underscreened populations and in LMICs.
Nevertheless, HPV self-sampling in LMICs might be associated with a number of ethical challenges, including concerns about autonomy, opportunity costs, and limited health care resources. For implementation of HPV self-sampling screening programs in LMICs to be successful, it is imperative to understand and address the opportunities and challenges of self-sampling so as to realize its substantial benefit to women’s health while limiting its potential harms.
Specimen Collection and Results Disclosure
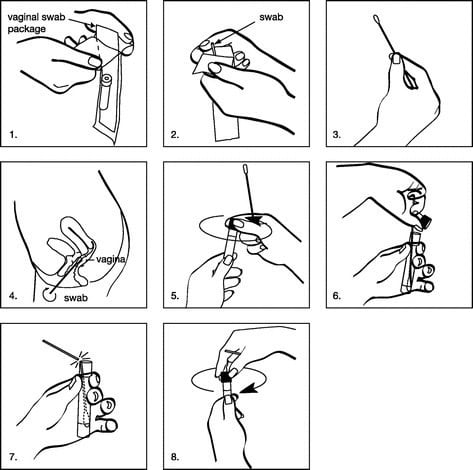
In the context of cervical cancer screening, the procedure for self-sampling is simple and does not require specific training (see Figure 1). Briefly, the woman is given a kit containing the necessary tools for self-collection, including a swab (or brush), a tube, and an envelope or zipper storage bag. To perform self-sampling, she chooses a private place (at home or at work) where she feels comfortable, takes off her underwear, and puts one leg on a chair or bench. She then holds the free end of the swab’s handle and gently pushes the other end to the top of the vagina. When the swab is inserted in her vagina, the woman turns the handle 2 or 3 turns, then removes the swab completely from her vagina, puts it into the tube, snaps the swab handle to break it, and caps the tube. Finally, she puts the tube into the envelope and seals it. The sealed envelope is either mailed to the laboratory or handed to a community health worker or health care practitioner who takes it to the lab. The procedure is easy and does not take more than 2 to 3 minutes. Generally, the laboratory is owned or equipped by the institution or entity that sponsors the cervical cancer screening program. In most Latin American and Asian countries, the implementation of HPV screening programs is mainly supported by governments,9,10 while in Africa, these programs are usually supported by nongovernmental organizations and research funds.11
Figure 1. Procedure for Self-Collected Vaginal Sampling
a Reprinted with permission from Wolters Kluwer.12
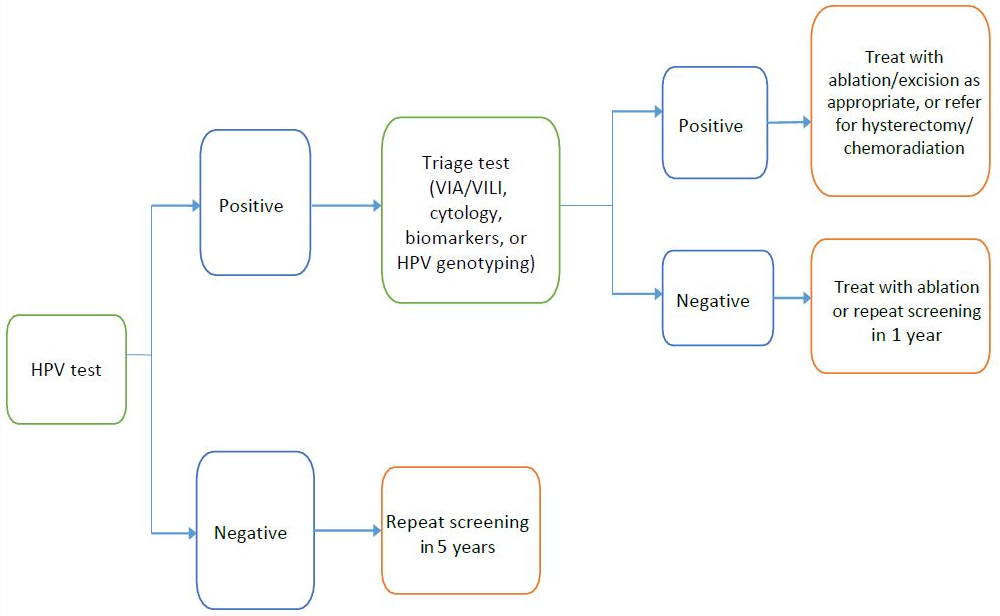
Processing and disclosing the results takes several steps (see Figure 2). In the lab, the technician processes the specimen contained in the tube, then runs the HPV test using an automated machine that provides results after a couple of hours (for rapid HPV analyzers). When the analysis is complete, the lab technician reads the result (positive or negative), which is returned to the woman via mail or through the community health worker or her health care practitioner. In any case, the screening result is generally accompanied by an interpretation of the result with recommendations about next steps. In the context of primary screening, a negative HPV test result indicates that the woman is at very low risk of developing cervical cancer within the next decade. She is therefore advised to repeat the test after 5 to 10 years. A positive HPV test result indicates that the woman has acquired the virus responsible for cervical cancer and might require further evaluation in a health care facility. Depending on the resources available and the appearance of the cervix, she might benefit from immediate treatment (with ablation or excisional therapy) or undergo additional workup, ie, a triage test—visual inspection with acetic acid (VIA) or visual inspection with Lugol’s iodine (VILI), cytology, biomarkers like OncoE6, or HPV genotyping—which may be complemented by colposcopy and/or biopsy (if available) to determine if she has a cervical precancerous or cancerous lesion that requires immediate treatment.
Figure 2. Proposed Cervical Screening and Treatment Algorithm With Primary HPV Testing for LMICs13
HPV indicates human papillomavirus; VIA, visual inspection with acetic acid; VILI, visual inspection with Lugol’s iodine.
Merits and Drawbacks of HPV Self-Sampling
Potential benefits. Self-sampling for cervical cancer screening might offer many benefits to women in LMICs. By respecting women’s privacy, self-sampling might encourage screening participation in underscreened populations and in LMICs. Although cancer screening consultation is generally sensitive, self-sampling allows for screening without undergoing pelvic examination. It has been reported that lack of privacy for women is one of the important reasons behind forgoing screening in LMICs.14 Further perceived barriers to screening include fear and shame, especially when it would involve unnecessary exposure of private parts in the presence of male health care practitioners,14 which might negatively impact women’s self-confidence. Women also need to be assured that the privacy of their results is maintained.15 Interestingly, HPV testing (especially polymerase chain reaction-based assays) was found to be as accurate on self-collected specimens as on clinician-collected specimens,16,17 suggesting that women can effectively replace health care practitioners in collecting samples for HPV testing. Health care practitioners, after adequate training and supervision, can safely provide management and follow-up of HPV positive women in primary care settings.7,18
Efforts to create awareness of women’s privacy rights should be directed at both women and clinicians. First, educational interventions aimed at raising women’s awareness of their duties and rights should be fostered in LMICS. Second, appropriate training of community health workers and health care practitioners would improve their understanding of patients’ rights to access and control information. Third, national or regional guidelines on cervical cancer prevention in LMICs should highlight policies that govern women’s privacy.
Other benefits of self-sampling for cervical cancer screening in LMICs include (1) superior clinical performance of HPV test compared to cytology or visual screening methods (VIA/VILI), allowing for the proper detection of cases of cervical cancer precursors; (2) potentially longer time interval between screening rounds (from 2 to 3 years with cytology or VIA/VILI to 5 years or more with HPV test), and (3) initiating screening at an older age (21 to 25 years with cytology or VIA/VILI vs 30 to 35 years with HPV testing), thereby reducing the number of screening rounds in a woman’s lifetime.19 Moreover, self-collected HPV testing has proven to be more cost effective than cytology in LMICs.20,21 Of note, in most limited-resource settings, women do not have health insurance, and health care expenditures are often paid out of pocket. For all these reasons, self-sampling is of value in LMICs, where unfamiliarity with the screening concept, lack of time, need for spousal permission, fear of financial burden, and fear of social marginalization are known obstacles to cervical cancer screening.7,22
Screening with HPV self-sampling is thus considered to be one of the most practical approaches for early detection of cervical cancer in LMICs, and it is the most effective in reducing the burden of disease at an affordable cost.19,20,21 Ethically, providing self-sampling as an alternative to other screening programs for prevention of cervical cancer in LMICs is a significant and reasonable act of beneficence.
Potential limitations. There are also potential limitations to adopting HPV self-sampling for cervical cancer screening in LMICs. Due to the high sensitivity of HPV testing, there is concern that it might lead to the overdetection of cervical dysplasia and thus unnecessary interventions (such as needless treatment, colposcopy, and/or biopsy) for both transient HPV infections and less serious cervical lesions that would have otherwise resolved on their own, subjecting those affected to unnecessary physical and mental burdens.23 This consideration is of utmost importance in LMICs, where there is a shortage of follow-up and treatment facilities as well as a lack of trained clinicians who can adequately manage and support HPV positive women.24 Thus, educating patients and practitioners and to some extent reinforcing health care infrastructures are major components of implementing HPV self-sampling in LMICs.
In addition to the HPV test’s potential for false positive results, HPV self-sampling poses potential challenges to the workflow of clinicians and laboratory specialists.25 The introduction of self-sampling might change the makeup of the services and workforce required in already resource-constrained settings. Indeed, facilities equipped with HPV machines might require (1) lab technicians who are trained to run the test and report the results; (2) community health workers who have been trained to properly explain the self-sampling procedure, adequately transport the self-collected specimens to the laboratory, and appropriately interpret and disclose the HPV results to women in the community; and (3) skilled clinicians to manage and follow up with women who tested positive. Implementing these changes would require decision makers to discuss and choose to respect the rights of women in LMICs to equal and appropriate treatment.
The fact that HPV is mainly transmitted through sexual contact might also affect how women interpret the screening results in ways that cause harm. While a negative HPV result might be perceived as a sign of reproductive health, some women who receive a negative test result (especially those with multiple previous or concurrent sexual partners) might consider themselves as being less vulnerable to the virus, and this false belief could induce them to engage in more risky sexual behaviors. Conversely, women might fear that a positive HPV test would bring them shame, blame, and even abandonment by their husbands and families, so some might prefer not to know the test result because of their fear of a positive result.26,27 Furthermore, women in patriarchal societies might fear the stigma associated with a positive result; for example, they might worry about male partners suspecting them of having other sexual partners.
Developing culturally appropriate messages and educational materials aimed at mitigating women’s feelings of guilt when HPV positive or feelings of invincibility when HPV negative might encourage women to participate in cervical cancer screening and might decrease the stigma of treatment. Such health promotion messages through face-to-face education with pictures and diagrams and through local media need to be aimed at both women and men.
Conclusion
HPV self-sampling as a global strategy for cervical cancer prevention is more respectful of women’s privacy and more accepted and cost effective than cytology and visual screening, and it has the potential to reduce social inequalities in access to screening in LMICs. However, it is associated with a number of policy and ethical concerns, including issues related to privacy of information, disclosure and interpretation of results, and potential harms of screening. These considerations need to be accounted for to successfully introduce self-sampling for cervical cancer screening at the community level in LMICs.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A.
Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries.CA Cancer J Clin.
2018;68(6):394-424.
Ronco G, Giorgi-Rossi P, Carozzi F, et al.
Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: a randomised controlled trial.Lancet Oncol.
2010;11(3):249-257.
Arrossi S, Thouyaret L, Herrero R, et al.
Effect of self-collection of HPV DNA offered by community health workers at home visits on uptake of screening for cervical cancer (the EMA study): a population-based cluster-randomised trial.Lancet Glob Health.
2015;3(2):e85-e94.
Crosby RA, Hagensee ME, Vanderpool R, et al.
Community-based screening for cervical cancer: a feasibility study of rural Appalachian women.Sex Transm Dis.
2015;42(11):607-611.
Fokom Domgue J, Ngalla C, Kakute P, et al. Feasibility of a community-based cervical cancer screening with “test and treat” strategy using self-samples for HPV testing: experience from rural Cameroon, Africa [published online ahead of print October 21, 2019]. Int J Cancer.
Racey CS, Withrow DR, Gesink D.
Self-collected HPV testing improves participation in cervical cancer screening: a systematic review and meta-analysis.Can J Public Health.
2013;104(2):e15-e166.
Gupta R, Gupta S, Mehrotra R, Sodhani P.
Cervical cancer screening in resource-constrained countries: current status and future directions.Asian Pac J Cancer Prev.
2017;18(6):1461-1467.
Tsu VD, Njama-Meya D, Lim J, Murray M, de Sanjose S. Opportunities and challenges for introducing HPV testing for cervical cancer screening in sub-Saharan Africa. Prev Med. 2018;114:205-208.
Chernesky M, Hook EW III, Martin DH, et al.
Women find it easy and prefer to collect their own vaginal swabs to diagnose Chlamydia trachomatis or Neisseria gonorrhoeae infections.Sex Trans Dis.
2005;32(12):729-733.
Allen-Leigh B, Uribe-Zuniga P, Leon-Maldonado L, et al. Barriers to HPV self-sampling and cytology among low-income indigenous women in rural areas of a middle-income setting: a qualitative study. BMC Cancer. 2017;17(1):734.
Chigbu CO, Aniebue U.
Why southeastern Nigerian women who are aware of cervical cancer screening do not go for cervical cancer screening.Int J Gynecol Cancer.
2011;21(7):1282-1286.
Polman NJ, Ebisch RMF, Heideman DAM, et al.
Performance of human papillomavirus testing on self-collected versus clinician-collected samples for the detection of cervical intraepithelial neoplasia of grade 2 or worse: a randomised, paired screen-positive, non-inferiority trial.Lancet Oncol.
2019;20(2):229-238.
Arbyn M, Smith SB, Temin S, Sultana F, Castle P; Collaboration on Self-Sampling and HPV Testing. Detecting cervical precancer and reaching underscreened women by using HPV testing on self samples: updated meta-analyses. BMJ. 2018;363:k4823.
Ginsburg O, Badwe R, Boyle P, et al.
Changing global policy to deliver safe, equitable, and affordable care for women’s cancers.Lancet.
2017;389(10071):871-880.
Fokom Domgue J, Valea FA. Is it relevant to keep advocating visual inspection of the cervix with acetic acid for primary cervical cancer screening in limited-resource settings? J Glob Oncol. 2018;4:1-5.
Campos NG, Mvundura M, Jeronimo J, Holme F, Vodicka E, Kim JJ. Cost-effectiveness of HPV-based cervical cancer screening in the public health system in Nicaragua. BMJ Open. 2017;7(6):e015048.
Termrungruanglert W, Khemapech N, Tantitamit T, Sangrajrang S, Havanond P, Laowahutanont P. Cost-effectiveness analysis study of HPV testing as a primary cervical cancer screening in Thailand. Gynecol Oncol Rep. 2017;22:58-63.
Brandt T, Wubneh SB, Handebo S, et al. Genital self-sampling for HPV-based cervical cancer screening: a qualitative study of preferences and barriers in rural Ethiopia. BMC Public Health. 2019;19(1):1026.
Hoste G, Vossaert K, Poppe WA. The clinical role of HPV testing in primary and secondary cervical cancer screening. Obstet Gynecol Int. 2013;2013:610373.
Denny L, de Sanjose S, Mutebi M, et al.
Interventions to close the divide for women with breast and cervical cancer between low-income and middle-income countries and high-income countries.Lancet.
2017;389(10071):861-870.
Fokom-Domgue J, Vassilakos P, Petignat P. Is screen-and-treat approach suited for screening and management of precancerous cervical lesions in sub-Saharan Africa? Prev Med. 2014;65:138-140.
Were E, Nyaberi Z, Buziba N.
Perceptions of risk and barriers to cervical cancer screening at Moi Teaching and Referral Hospital (MTRH), Eldoret, Kenya.Afr Health Sci.
2011;11(1):58-64.
Dabash R, Vajpayee J, Jacob M, et al. A strategic assessment of cervical cancer prevention and treatment services in 3 districts of Uttar Pradesh, India. Reprod Health. 2005;2:11.